
‘‘For many smokers, a genuine desire to quit and, if necessary, persistent and repeated attempts to quit may be all that is necessary.”
Everett Koop, Surgeon General, May 1998
Nicotine is named after Jean Nicot, the French ambassador to Portugal from 1559 to 1561. He is credited with bringing tobacco plants and seeds back to France, and for introducing snuff to the French royal court. It was extracted from tobacco in the early 1800s, and the chemical formula of the substance (C10H14N2) was determined by the 1840s. It is an alkaloid that is found in the nightshade family of plants, mainly in tobacco. It is also present in low quantities in tomatoes, potatoes, cauliflower, aubergines and green peppers.
Nicotine can be poisonous in its pure form. Reports dating back to the sixteenth century suggest nicotine poisoning from the “therapeutic” use of tobacco-infused enemas. It is not, however, lethal in the doses typically found in cigarettes.
In the first Surgeon General’s Report on Smoking and Health in 1964 deemed the tobacco habit to be “an habituation rather than an addiction, in conformity with accepted World Health Organisation definitions, since once established there is little tendency to increase the dose; psychic but not physical dependence is developed; and the detrimental effects are primarily on the individual rather than society.” (p354, emphasis in the original).
It was not until 1988, when Everett Koop was Surgeon General, that nicotine was deemed “addictive” and, moreover, that “the processes that determine tobacco addiction are similar to those that determine addiction to drugs such as heroin and cocaine”. This has subsequently often been repeated as “nicotine is as addictive as heroin” although that is not what was actually stated.
The World Health Organisation’s definition of “addiction” is as follows:
Repeated use of a psychoactive substance or substances, to the extent that the user (referred to as an addict) is periodically or chronically intoxicated, shows a compulsion to take the preferred substance (or substances), has great difficulty in voluntarily ceasing or modifying substance use, and exhibits determination to obtain psychoactive substances by almost any means. Typically, tolerance is prominent and a withdrawal syndrome frequently occurs when substance use is interrupted. The life of the addict may be dominated by substance use to the virtual exclusion of all other activities and responsibilities. The term addiction also conveys the sense that such substance use has a detrimental effect on society, as well as on the individual; when applied to the use of alcohol, it is equivalent to alcoholism. Addiction is a term of long-standing and variable usage. It is regarded by many as a discrete disease entity, a debilitating disorder rooted in the pharmacological effects of the drug, which is remorselessly progressive. From the 1920s to the 1960s attempts were made to differentiate between addiction; and “habituation”, a less severe form of psychological adaptation. In the 1960s the World Health Organization recommended that both terms be abandoned in favour of dependence, which can exist in various degrees of severity. Addiction is not a diagnostic term in ICD-10, but continues to be very widely employed by professionals and the general public alike.
The description of addiction from WHO is interesting in a number of respects: addiction is not a diagnostic term but one of common parlance; addiction conveys the sense of a detrimental effect on society; addicts may be dominated to a point of virtual exclusion of all other activities; there is great difficulty in modifying use; the user is “intoxicated”; tolerance is “prominent” meaning that a higher dosage is required to achieve the same level of response.
Returning to the 1964 Surgeon General’s report (p350) there is a useful characterisation of what was meant at the time as the similarities and important differences between addiction and habituation.
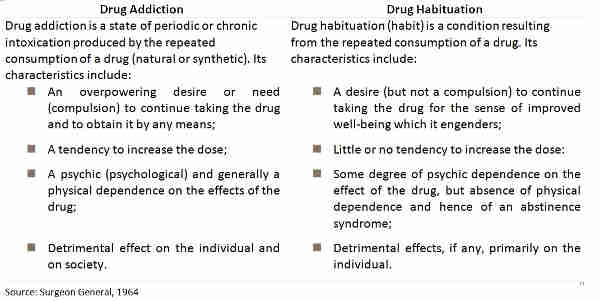
Table 4: Drug addiction and drug habituation
Even a non-smoker can readily see that tobacco is unlikely to meet the hurdle for “addiction” as described above. It is readily accepted that quitting smoking can be difficult, but there are as many ex-smokers in the UK and the US as current smokers, suggesting that many have met the challenge. It is not clear that smokers display “tolerance” as average daily consumption has been declining for many decades. “Social smokers” demonstrate that use can be modified according to circumstances, whether that is abstinence in the early part of a week or increased consumption in a social setting. The question of the “societal” cost of smoking is dealt with in more detail below.
The Surgeon General commented in 1964 (p352) “In contrast to drugs of addiction, withdrawal from tobacco never constitutes a threat to life”. As the opening quotation from Everett Koop suggests, despite his comparison of nicotine to cocaine, his own view was closer to that of the 1964 report. It appears that “the message” that smokers should quit was more important than the science, once again.
Of course the classification of smokers as “addicts” is important in other ways. By classifying smokers as addicts, it removes from them the liability of personal choice. It is no longer the smoker’s fault that they are a smoker it is the fault of the tobacco companies (“Big Tobacco”). It also means that regulation and taxation of their habit can be undertaken “for their own good” because they are clearly in the grip of a force greater than their own free will and cannot be trusted to make their own decisions with regard to their health.